BACKGROUND: Acute exposure to hypobaric hypoxia can give rise to acute mountain sickness, and rarely, high altitude pulmonary edema, and high altitude cerebral edema. However, with gradual adaptation to “chronic hypoxia”, following the Adaptation to High Altitude Formula (Adaptation = time / altitudeΔ), the organism does remarkably well. High altitude residents are perfectly adapted to their environment. The cities of La Paz (3100–4100 m) and El Alto (4100 m) stand as living proof of this with 2.7 million inhabitants living perfectly normal lives, undisturbed by hypoxia and most even unaware of its existence. All the cells of the organism adapt to a lower arterial oxygen arterial partial pressure (PaO2) and likewise to a lower arterial partial pressure of carbon dioxide (PaCO2), an essential component that linked to an increased compensatory hemoglobin explain the paradox of increased “tolerance to hypoxia” at high altitude.
METHODS: We reviewed the > 70 years old population historic records of the official Bolivian registration service SEGIP. Two groups were analyzed: those greater than 90 years of age, and those greater than 100 years of age according to the different altitude departments in Bolivia.
RESULTS: As the altitude increases, the longevity increases. Santa Cruz at 416m and La Paz at 3800m (average), both with around 2.7 million inhabitants each, have 6 versus 48 centenarians respectively.
CONCLUSIONS: Life under chronic hypoxia is not only tolerable, but also is, in fact, favorable to improve or treat many pathological conditions such as asthma, coronary artery disease, obesity and even giving rise to improved longevity. Sea level residents (when compared to high altitude residents) suffer a disability: poor tolerance to hypoxia.
Keywords: Adaptation, high altitude, hypoxia, longevity, tolerance to hypoxia
| How to cite this article: Zubieta-Calleja GR, Zubieta-DeUrioste NA. Extended longevity at high altitude: Benefits of exposure to chronic hypoxia. BLDE Univ J Health Sci 2017;2:80-90 |
| How to cite this URL: Zubieta-Calleja GR, Zubieta-DeUrioste NA. Extended longevity at high altitude: Benefits of exposure to chronic hypoxia. BLDE Univ J Health Sci [serial online] 2017 [cited 2023 May 30];2:80-90. Available from: https://www.bldeujournalhs.in/text.asp?2017/2/2/80/220947 |
Ever since casualties occurred during the first balloon ascents and likewise, the description of mountain sickness by Father Acosta in the Andes, and other Chinese ancient scripts, high-altitude sickness gave rise to a systematic fear to hypoxia.[1] Consequently, it became evident that going high could make people sick. And, this sickness could be felt through very unpleasant symptoms such as headache, shortness of breath, and vomiting that have been termed acute mountain sickness. Some cases evolved severely and were the cause of death with high-altitude pulmonary edema (HAPE) and/or high-altitude cerebral edema. Furthermore, modern flights in pressurized cabin aircrafts at 10,000 m of altitude with sudden decompression can give rise to death due to asphyxia resulting from sudden extreme hypoxia, much like removing a fish from water. Hence, the overall impression that remains about hypobaric hypoxia is that it is bad and detrimental to health.
The normal increase of the hematocrit in high-altitude residents (relative to sea-level values) was originally described by Viault.[2],[3] Carlos Monge Medrano then observed some cases where the hematocrit was higher than those of normal residents and called this chronic mountain sickness (CMS).[4],[5] The original terminology was polycythemia, but it became evident that the term also referred to all three types of cells in blood: red blood cells, white blood cells, and platelets, an inadequate and imprecise terminology. Hence, since the white blood cells and platelets were not increased, the name was changed to erythrocytosis and then evolved in the scientific community to excessive erythrocytosis. Yet, these terms are also inaccurate as the red blood cells are not altered as the Greek “osis” would imply, hence the new precise terminology is polyerythrocythemia (PEH) that can be expressed as poly-erythrocyt-hemia.[6]
“Polycythemia” was originally defined as a “loss of adaptation” or “de-adaptation” of high-altitude residents. CMS was then considered a high-altitude “disease” or “sickness,” i.e., an independent pathological entity. We question: How can an increase of red blood cells (PEH), a simple sign in medical terms, always associated to a low partial arterial oxygen tension (PaO2), be considered a sickness? Analogously, jaundice, a medical sign of several hepatic and hematological diseases, is merely a medical sign and can never be considered a “disease.” Some even suggested that long-term residence at high altitude would lead to CMS.[7] This would imply that the cities of La Paz 3100–4000 m, El Alto 4100 m, Lhasa 3600 m, and other high-altitude cities would be “filled” with the so-called CMS in their elders. This is definitely, not so, and as an example, Gustavo Zubieta-Castillo (Sr.) who established these reflections and new concepts passed away reaching 90 years of age and maintaining his normal hematocrit of 50% throughout his life, being born and living at high altitude in the city of La Paz (3600 m). During the consensus statement on diseases at high altitude,[8] we had a dissenting point of view and after much discussion, the use of the term “loss of adaptation” was finally dropped; however, the inadequate use of terms “de-adaptation” and “loss of adaptation” remain up-to-date. And, it continues to be used today in spite of the publications that strongly criticized its use.[9],[10],[11] The sentence “The organic systems of human beings and all other species tend to adapt to any environmental change and circumstance within an optimal period of time, and never tend toward regression (loss of adaptation) which would inevitably lead to death”[6] has not been clearly understood or is simply being ignored.
Many have jumped into searching for a genetic change of “de-adaptation” as an opposing point of view from the Tibetan adaptation where the hematocrits are lower than those of Andes residents. This is attributed to multigenerational residence at high altitude. Several other parameters such as higher SpO2 during sleep and lower incidence of pulmonary hypertension have also been found in Tibetans.[11] Hence, it can be clearly understood that this would be considered a model for optimal high-latitude genetic adaptation. On the other hand, CMS would be considered the opposite stance (i.e., inadequate adaptation). However, poor understanding of the causes of the increase of the hematocrit and hemoglobin beyond the normal-resident values gave rise to a wrong interpretation, generating confusion regarding this sign (the increase of red blood cells, i.e., poly-erythro-cythemia) that should not be considered a “sickness,” but rather the response of the organism to multiple diseases fundamentally, pulmonary and cardiac, but not excluding other organs.[12] Additionally, there is a fear of an increase of the number of red blood cells, assuming it would produce thromboembolism.
Furthermore, several studies showed that high-altitude residents’ newborns have lower birth weights which has been implicated in qualifying hypoxia as deleterious.[13] Nevertheless, current observations in Cerro de Pasco 4300 m, Cusco, and others show normal birth weights.[14],[15] Other studies in pregnant animals exposed to hypoxic environments in chambers have shown that the offspring have very striking anomalies in the pulmonary vasculature,[16] however the just-pregnant sea-level animals were exposed acutely to extreme hypoxia 5000 m without any adaptation. A situation that could be compared to an acute hypoxia in a normal pregnancy, as happens in eclampsia.
Reproduction in humans in cities such as El Alto, Bolivia, at 4100 m is very successful and gives rise to the fastest growing population in Bolivia, a multi-altitude country. Another example is the case of Samuel Mendoza, who is in charge of the refuge in Chacaltaya at 5250 m, a ski resort (that has lost its purpose due to ice melting secondary to global warming), and has been working there for over 34 years. He goes up every day and has often slept there. He is currently 57 years old and his health is optimal with a normal heart size. He has gained notoriety by a recent film named “Samuel in the Clouds” by director Pieter Van Eecke.[17] His niece also worked there and remained at 5350 m throughout her pregnancy back in 1993. She gave birth at 5200 m, to a healthy baby, currently in her twenties and who lives, studies, and practices sports in El Alto (4100 m). They were presented during the International Conference of High Altitude (CIMA) held in La Paz, Bolivia, in February 2016. They are a living and successful example of adaptation and reproduction at high altitude.
With the clearly negative point of view in relation to life at high altitude (with which we disagree, as lifetime high-altitude residents), we ran into a newspaper publication of the oldest man alive in the Bolivian High Plateau Altiplano (4000 m). He had been described as having 123 years of age.[18] So, the hypothesis arose “Does man live longer at high altitude?”
We asked Servicio General de Identificacion Personal (SEGIP), i.e., General Service of Personal Identification, the institution that manages all the identification records in Bolivia, to forward us the ages in relation to altitude of residence. They reported all individuals older than 70 years from two different databases in all the Bolivian population. On the one hand, consolidated registrations at SEGIP informing of 177,571 living citizens and on the other hand historical catalog records from 70 to 130 years old.
These data were cataloged in relation to the nine departments (political division of Bolivia) that are located at different altitudes, ranging from 221 m of altitude in Pando all the way to 4090 m in Potosi. [Table 1] shows the latest census data, and the data provided to us by the SEGIP.
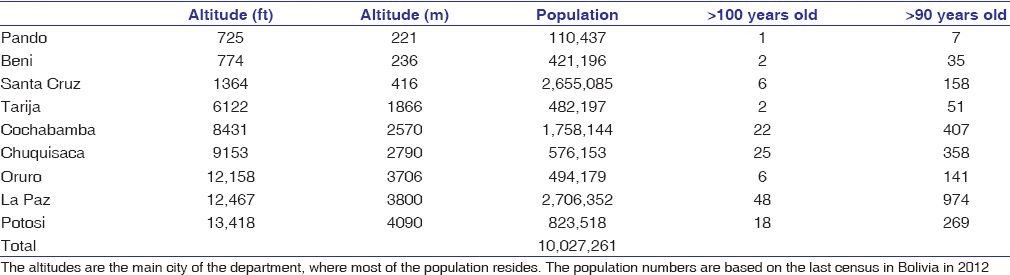
The altitudes are the main city of the department, where most of the population resides. The population numbers are based on the last Census in Bolivia in 2012.
It is noteworthy to consider that each department has different altitude ranges, but the report from SEGIP included different municipalities so that one can appreciate the true altitude of residence. To describe true longevity, it was seen convenient to report on those older than 90 and 100 years old, as these extreme ages are reached only by a few citizens in any part of the world. The intention is to make a comparison between different altitudes of residence.

It becomes irrefutably evident that longevity is indeed greater at high altitude than at lower altitudes in Bolivia. The higher the altitude of residence, the greater the longevity in Bolivia. Two departments (analogous to states) with similar populations close to 2,700,000 inhabitants are compared for illustrative purposes: the department of Santa Cruz located at 416 m of altitude in the tropical areas of Bolivia and the neighboring cities of La Paz and El Alto, situated in the high-altitude department of La Paz, between 3000 m and 4100 m, approximately. The difference is statistically significant, with 6 individuals older than 100 years old in Santa Cruz versus 48 in La Paz. When individuals older than 90 years were compared, there were 158 in Santa Cruz versus 974 in La Paz. Interestingly, individuals older than 100 years were 8 times higher at high altitude in La Paz, than in Santa Cruz. Whereas individuals older than 90 years of age were 6 times more at high altitude than at sea level. This implies that there is a higher ratio as age advances. The life expectancy of the overall population in Bolivia is 68.34 years of age, as of 2014, but this is due to many other factors typically present in a developing country.
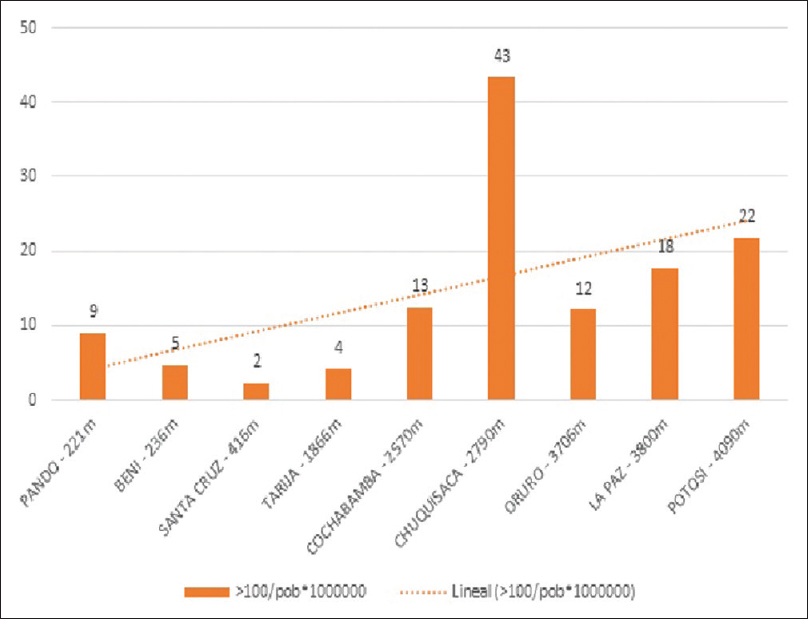
Chuquisaca, situated at 2790 m, has the highest number of centenarian residents when adjusted to population [Figure 2], and this is probably due to other factors such as a good healthy nutrition, based on natural products plus pleasant weather, less pollution and less stress from life as that present in busy cities such as La Paz, among other things. This is a very good example where other variables are frequently overlooked when exclusively attributing observations to high-altitude hypoxia. Hypoxia is often blamed for every abnormality, not considering the fact that many aspects of life in high-altitude cities around the world have been neglected. Such is the case of lack of hygiene, lack of education, lack of nutrition, lack of medical care, overexposure to pollutants and sources of infection, exposure to cold weather, and unsuitable living quarters, among others. It is important to remember that the first cause of death in developing countries such as Bolivia, is infectious diseases, as opposing the cardiovascular pathologies at sea level in the most developed countries. At high altitude, the incidence of patent ductus arteriosus, is slightly higher than at sea level.[19] Interestingly, there is supposedly a higher tendency of developing cardiopathies from early intra-uterine growth, at sea level.[20] Since the intention is to see things objectively and scientifically, with a critical eye, the diagnosis of medical, environmental, and circumstantial events has to be precise.
To explain longevity, it is necessary to look into several parameters that would explain it: genetics, diseases, physical stress, nutrition, biological responses to hypoxia, tolerance to hypoxia, lower CO2 levels and less O2, less aggression of reactive oxygen species (ROS), increased number of mitochondria, and others. Accidents and trauma can possibly be excluded from this analysis as they would not be so different at different altitudes.
First of all, there are genetic characteristics. This undoubtedly is the most transcendental factor, as the Geriatric Society has well established.[21] It is interesting to note that women have a longer lifespan than men, although men have always been classified as the “stronger” of the two genders. One could be tempted to argue that muscles have a negative influence on longevity and perhaps that a more sedentary life could help. Genetic studies giving clues regarding longevity show the complexity of interpretation,[22] yet they could perhaps be beneficial to help explain the findings in this paper.
Second, one can consider the physical characteristics of the environment. There is a wide variety of tropical diseases, which high-altitude inhabitants are protected from. These include dermatological conditions such as tungiasis (sand flea disease), cutaneous larva migrans (creeping eruptions), allergic exanthema, myiasis, dracunculiasis and onchocerciasis, as well as Buruli ulcer, sporotrichosis, and tinea fimbricata, which can be attributed to various fungi, protozoa, and ectoparasites, along with their vectors, that mainly flourish in places with a warm and humid climate. At high altitude, there are no mosquitoes and hence high-altitude residents are free from malaria, yellow fever, chikungunya, dengue, Eastern Equine Encephalitis, St. Louis Encephalitis, LaCrosse Encephalitis, Western Equine Encephalitis, West Nile Virus, and others.
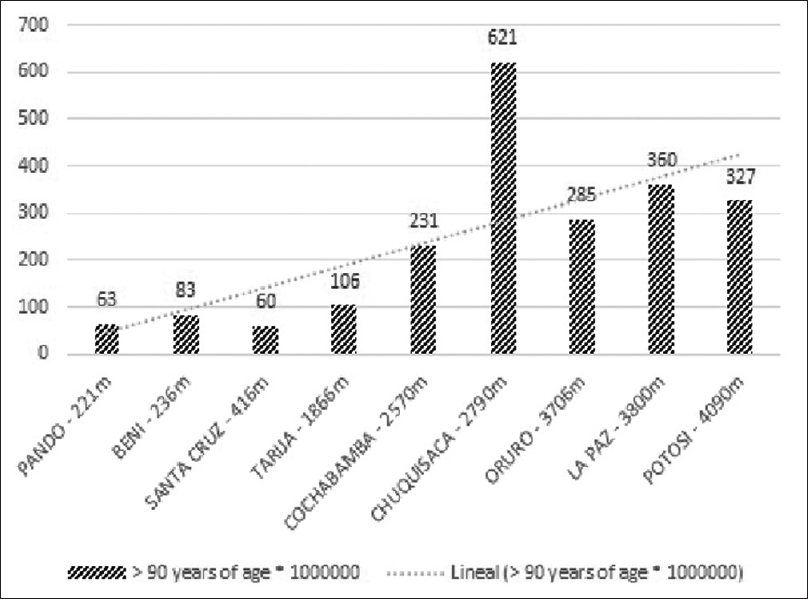
Although several of these are present in other latitudes or longitudes, still at sea level, parasitic infestations such as Leishmaniasis, Chagas’ disease, echinococcosis, and Elephantiasis (Lymphatic filariasis) are also inexistent at high altitude. There is also a greater incidence of fungi at sea level, due to the humid environment and higher temperatures, whereas at high altitude, the air is dry and temperatures are lower. Tropical diseases also contribute to cardiovascular conditions. For example, trypanosomiasis, primarily found in tropical climates, can often complicate into chagasic cardiomyopathy, which is associated with heart failure, embolism, arrhythmia, and stroke. Interestingly, as shown in [Figure 2] and [Figure 3], Chuquisaca (also known as Sucre), an endemic area for Chagas, has the greater longevity at 2790 m.
Endomyocardial fibrosis, a condition causing restrictive cardiomyopathy, also includes various helminthic parasites in its etiology, and is associated with pericarditis and mural thrombi. Chronic hepatosplenic schistosomiasis, caused by helminth schistosoma, leads to pulmonary hypertension and cor pulmonale.[23] Besides, a significant proportion of casualties occur in tropical regions by dangerous fauna of the area. Many marine organisms release toxins such as saxitoxin and domoic acid, which directly affect the brain. There is also a potential risk of coming in contact with amphibians, insects, and other reptiles which are typically native of warm wet climates, such as scorpions, spiders, snakes, and toads, whose venoms can cause severe neurologic and cardiologic damage.
All these conditions cause significant morbidity and mortality that can reduce lifespan. Furthermore, the temperatures in the high-altitude cities of Bolivia, due to its proximity with the equator, are quite pleasant and not extreme, except in very few places in winter times. One of the factors that contributes to this nice weather is the sun, present throughout the whole winter. This kind of climate provides an unfavorable environment for all these tropical diseases, thus protecting the residents from disease and distress and thus enhancing their productivity and longevity significantly.
Moreover, increased solar radiation possibly helps the body to enhance the synthesis of Vitamin D which has been shown to have beneficial effects on the heart and some cancers.[24] In another study by Voss et al. that was aimed at assessing whether high-altitude residents confer any benefit of lowering obesity rates among those at a high risk of becoming obese, it was concluded that residents stationed at high altitudes had a lower hazard ratio of incident obesity diagnosis, as compared to low-altitude residents. Thus, chronic hypoxia confers long-term protection from obesity and subsequently its associated comorbidities.[25]
Third, at high altitude, ultraviolet (UV) radiation exposure is highly increased. In a comparison between the cities of Copenhagen at sea level and the city of La Paz (3100–4100 m), it was shown that the highest UV-index/month (WHO 2006 classification) was classified as moderate 6 in the former whereas it was 18 in the latter classified as extreme. Long-term exposure to high altitude in residents was thought to have negative effects on the eye, so we undertook a study of the lens of residents after 35 years of life at high altitude, while staying temporarily in Copenhagen. Ophthalmologic studies showed that there was no difference in luminescence with respect to sea-level residents.[26] The eye adapts to high levels of UV radiation. Skin cancer is said to have a higher incidence, but no scientific reports have statistically proven this as far as we know. Many internet articles affirm that the incidence at high altitude due to UV radiation should be higher,[27] but no scholarly articles prove it. In fact, the Lancet affirmed [28] “Paradoxically, outdoor workers have a decreased risk of melanoma compared with indoor workers, suggesting that chronic sunlight exposure can have a protective effect.” This is why high-altitude residents have darker skins, in their natural and healthy adaptation to high altitude. We do not have rickets disease, suggesting that abundant sun exposure could be beneficial at high altitude, and maybe even therapeutic for some diseases. Two of the authors resided during 3½ years in Copenhagen, Denmark, at sea level, and presented multiple dental cavities as compared to their permanent high-altitude residence, where the incidence is much lower. It can be deduced that the higher levels of UV radiation at high altitude have little or no negative effect and perhaps quite the contrary have rather a positive effect on health. UV rays have sterilizing effects on bacteria and it is highly probable that they are beneficial at high altitude.
Fourth, the incidence of lung cancer has been shown to be much lower at high altitude than at sea level.[29] In fact, those authors go on boldly, based on a great number of scientific citations, to propose the hypothesis that oxygen is the cause of lung cancer. In a study, on the incidence of lung cancer at the Instituto Nacional del Tórax (National Thorax Institute) in the city of La Paz performed back in 1980, out of a 10-year span of diagnosis reviews, we found only three cases of lung cancer. This information was not published, at the time, since the abnormally low levels in an institution that cares for chest diseases at 3500 m, we assumed, would have been questioned.
Another interesting observation is that lung disease is different at high altitude. The air is dry and this has been, even from the past century, considered beneficial to treat lung disease, even pulmonary tuberculosis (TB) in the well-known mountain medical resorts in Europe. The thin, dry, and reduced pollen in the air can indeed reduce the incidence of extremely aggressive sea-level diseases such as asthma. In a research carried out by Eisen et al., which used mycobacterial luminescence to assess colony count and comparison with growth at low-altitude controls, it was inferred that ascent to or residence at high altitudes was associated with reduced growth of the organism, as well as augmentation of antimycobacterial cellular immunity.[30]
According to an article entitled “High altitude treatment of Pulmonary Tuberculosis” by Amrein, dating to the year 1929, the high-altitude climate acts like a “stimulant or tonic” for the treatment and rehabilitation of TB patients; owing to beneficial elements, like dry air and abundant sunshine. Children were said to be benefited especially, and the cases had reportedly shown significant improvement in their condition.[31]
In our medical practice in the city of La Paz, we observed very few cases or isolated cases of asthma. The children of diplomats who suffer constant hospitalizations with severe asthma crisis and permanent use of bronchodilators, inhalers, and inhaled corticosteroid treatments at sea level frequently find that upon arriving to La Paz, the asthma disappears. In fact, the head of the main Intensive Care Unit at the Hospital Obrero in the city of La Paz 3500 m, Dr. Freddy Sandi, has affirmed that in his over 30 years of practice he has never seen or treated a case of asthma crisis. Colleagues that at sea level suffer asthma and regularly use medication, have on attending our Chronic Hypoxia Symposiums in La Paz, dropped their medication and their respiratory status was significantly improved.
At high altitude, we neither see pink puffers, nor blue boaters. The incidence of emphysema as that seen at sea level is certainly much lower or rather nonexisting. Some people smoke too much, of course, but although it is evident that there are individual reactions, the chronic hypersecretory coughing patients are not very common. Various infections with pulmonary involvement, such as melioidosis, paragonimiasis, gnathostomiasis, and tropical eosinophilia, are also unlikely to occur, owing to the climate.[32]
Even coughing at high altitude has different characteristics. The rough-coarse thick coughs commonly heard at sea level (even in transportation media) are uncommon or very rare at high altitude. A dry environment with much lower quantities of mold is certainly favorable. Bread loafs left unused at high altitude only develop mold after a couple of weeks if they actually do not dry up and become hard.
One of the most significant studies in this regard is entitled “Effects of High altitude on Incidence of Common Diseases in Man,” that was carried out on a cohort of 20,000 Indian soldiers stationed at altitudes between 3692 and 5538 m (where temperature ranged from −19°C to 13°C, with almost no rainfall) and contrasted with 130,700 soldiers on plains between sea level and 760 m (where temperature ranged from 7°C to 41°C, with sufficient rainfall). Differences in morbidity rates over a period of 7 years were tabulated for both the groups of soldiers, and later graphically plotted for comparison. The diseases evaluated included infectious diseases such as mumps and pneumonia, diabetes mellitus, asthma, skin diseases, and rheumatoid arthritis, among many others. It was noted that most of the diseases taken into consideration showed significantly lower morbidity rates at high altitudes, than those at lower altitudes.
Factors such as reduced PaO2, lesser pollution, increased solar radiation, and reduced temperatures result in clinically relevant physiological changes, such as increased vital capacity, cerebral and peripheral blood flow, and lung ventilation. On chronic exposure, there are numerable adaptive mechanisms, such as improved respiratory function, adrenal hormonal function, thermoregulation, and blood production; along with reduced gastric acid secretion. These changes have been successfully put to therapeutic use for various ailments, by either natural or simulated high altitude.[33]
Fifth, in relation to sports, the world records in bicycle track speed racing are often broken at high altitude. The top 4 speed records were won at high altitudes of Aguas Calientes, Mexico, at 1880 m (flying 200 m time progression, 1 Km time trial progression, and team sprint progression) and La Paz, Bolivia, 3400 m (500 m time trial progression).[34] We believe that even the world record of 100 m dash could be improved at high altitude, because there is less resistance in the environmental air. The outstanding performance of the soccer (football) players at the summit of Mt. Sajama 6542 m, in 2001, was performed by skinny, not very tall, porters and guides of the town of Sajama and the city of La Paz [Figure 4]. They climbed from the base of Sajama at 4000 m to the summit 6542 m in 9 h, carrying the goal posts, their team shirts, and shorts and several red or orange painted-colored balls. They drew the pitch, played 20 min per side, tied 2–2, and came down in 6 h to celebrate in the town of Sajama.[35] When we planned this game, many people said that it would be a grave risk and that the players could die. They all performed very well, as is evident on the videos online. This proved the extraordinary capacity of man to perform even in very hypoxic environments, with adequate adaptation and training.

Their example was one contributing factor for the affirmation that man can adapt to life even in the extreme hypoxic environments like the summit of Mt. Everest.[36],[37] Avoiding the cold, getting good nutrition, and a very gradual and good adaptation to different increasing altitudes are essential. Other contributing factors to this theory included the very low levels of oxygen in arterial blood PaO2 of 35 mmHg or less in patients suffering from PEH at high altitude, normally present, likewise in uterus and during birth fetal PaO2 levels of around 29 mmHg. Also contributing was a case of HAPE, in a Portuguese Rugby player, that tolerated PaO2 levels of 29 mmHg in the city of La Paz at 3500 m, for a couple of days, that later on fully recovered and continued to play at sea level.
Death in Mt. Everest climbers is often mistakenly attributed to high-altitude hypoxia, disregarding the other factors, such as fatigue, malnutrition, dehydration, and extreme cold environmental conditions. Only 9% of the deaths on Mt. Everest are due to high-altitude illness. Maybe even less, as most are on the way down, after exhaustion, extreme cold, and bad weather conditions that all are aggravating factors.[38] It was cold weather that defeated Napoleon and Hitler in Russia, obviously at sea level, and not hypoxia. It was extreme cold, exhaustion, and starvation, in very poor weather conditions and to some degree, perhaps deception that killed Robert Falcon Scott upon returning from the South Pole and learning that the Norwegian Roald Amundsen had gotten there first. It was by no means hypoxia, and by no means high-altitude hypoxia, but if the events would have happened in a mountain, hypoxia would most probably be blamed.
Sixth, back in 1964, observations in isolated perfused dog’s hearts at 3500 m showed that the heart was more resistant than at sea level.[39],[40],[41] On the other hand, cardiac rehabilitation is improved at high altitude or with the use of hypobaric chambers inducing hypoxia according to several studies.[42] Several outstanding studies are looking for the biochemical pathways that explain the increased resistance of hypoxia-exposed myocardial tissue.[43],[44] Postcardiac bypass patients’ rehabilitation was accelerated by altitude hypoxia, both performing mountain climbs and chamber-induced hypobaric exposure.[42] In a study conducted at the University of Colorado, it has been found that people living at high altitudes have a lower chance of dying from ischemic heart disease and tend to live comparatively longer, since low oxygen levels spur certain genes, which possibly affect cardiac function and create new collaterals to the heart, thus improving blood flow toward it.
It is interesting to point out that supplemental oxygen therapy in patients with ST-elevation-myocardial infarction without hypoxia may increase early myocardial injury and was associated with larger myocardial infarct size assessed at 6 months,[45] although this was to some degree questioned.
Overexposure to oxygen is usually avoided in stroke and cognitive enhancement therapy treatments, as well as in premature neonatal intensive care, which can otherwise lead to retrolental fibroplasia. Prolonged exposure to high oxygen levels may also cause pulmonary, cerebral, and ocular toxicity, which are not present at high altitudes. Similarly, the deleterious effects of oxidation of metal, seen in cars at sea level, are not observed at high altitude and our cars at high altitude in the city of La Paz have a longer lifespan as the oxidation is minimal. And certainly, physical objective observations can also be applied to biological adaptation, as the physical laws of matter apply to all altitudes, environments, and all the biological beings on planet earth.
It is well known that upon the initial exposure to a high-altitude environment such as the city of La Paz (4100–3100 m), newcomers can lose close to 4 or 5 kg. However, as adaptation takes place, the weight is partly if not all, recovered. Until a few years back, obesity and overweight were very uncommon in high-altitude cities. However, it has been recently observed that this is changing possibly due to fast food restaurant presence and high-carbohydrate diets. Diabetes and other metabolic diseases that had lower incidences are also increasing concomitantly, of course. Much like the importation of Polio to America during the Spanish Colony, nowadays, globalization brings these metabolic diseases even to high-altitude cities.
High-altitude adaptation has been defined as the optimal level of hematocrit, where red cells take the leading role, a more efficient energy-saving mechanism, replacing the extra effort of the heart and the lungs on acute exposure.[46] This hematocrit increase has been often referred to, by sea-level physicians, as deleterious. Our personal experience over many years shows that higher hematocrits are allies and not “dangerous.” We have searched for true evidence of increased risk of stroke in these patients at high altitude and we were unable to come up with solid proof in the bibliography. The presence of hypertension, cardiac arrhythmias, deep vein thrombosis, pulmonary thromboembolism, and alterations of coagulation among other comorbidities certainly increases the risk of stroke, but these are other aggravating factors and cannot be attributed to hypoxia alone.[6]
Quite the contrary to common belief, hypoxia is best tolerated at high altitude than at sea level.[47] The tolerance to hypoxia formula shows that tolerance on the summit of Mt. Everest can be up to 6 times better than at sea level.
Seventh, longevity could be explained in terms of healthier diets at high altitude. Products, cultivated in the high altitude fields like quinua are known for their high protein and effective nutrition. Likewise potatoes, “habas,” (a type of beans) white corns, onions, green peas. High altitude residents in La Paz also have abundant access to orange, tangerines, and bananas from the nearby tropical areas. Bolivians also eat meat regularly. Similarly, in the Himalayas, the diet of the inhabitants includes milk of yaks, which is very rich in vitamins and minerals (macro minerals as well as trace nutrients), as well as local crops such as amaranth, which is rich in proteins, manganese, and lysine, with cholesterol-lowering properties; buckwheat, which is rich in “rutin,” is said to promote the maintenance of cardiovascular health and prevent diabetes, and finger millets which are considered a “superfood,” since they are packed with nutrients and fiber.
More so, access to quality medical care is scarce in many Altiplano (high plateau) towns, but in spite of this, longevity is a fact. In the city of El Alto at 4100 m with over 1 million inhabitants, on the celebration of the 25th anniversary a few days back, the oldest resident was presented, a lady of 106 years of age in excellent health conditions.
Eight, Denham Harman originally proposed the “free radical theory of aging” in 1956, later refined to the “mitochondrial theory of aging” in 1970s.[48] The common theme in both was that oxidative damage accumulates with age; inclusion of the latter implicated ROS generated by mitochondria as the primary source of this stress. The focus in the redox biology field has now shifted to understand why and how the “quality” of the mitochondrial population in cells declines with age and integrates concepts from autophagy, cell signaling, and bioenergetics.[49],[50] Of particular interest is autophagy and mitochondrial biogenesis since they are both biological pathways that can link caloric restriction with healthy aging and bioenergetics.[51] The native residents at high altitude tend to have caloric restriction due to their environmental specific food resource. It is well known that at high altitude, there is a greater number of mitochondria as a result of adaptation. So, a greater number of mitochondria in well-adapted residents at high altitude throughout life could certainly aid in explaining longevity. Although Harman’s theory has apparently been questioned, we find that our statistical population fact-based analysis, here in Bolivia, shows that he had a point, a very real one.
It is interesting to note that oxidation lapses in cell studies seem more deleterious than hypoxic lapses as personally referred by Jan Marino Ramirez of the Center for Integrative Brain Research of the Seattle Children’s Hospital.
Nine, altitude can have a significant influence on athletic performance. A training modality called “Live High Train Low” was developed, according to which athletes can improve their performance by spending most of their time living at high altitudes but training at lower heights. Studies by Dufour et al. have proved that intermittent hypoxia training improves aerobic performance capacity [52] (submaximal and maximal running velocity and oxygen consumption rate), as well as mitochondrial function.[53] These effects are supposed to be mainly mediated by augmented red cell volume or erythropoiesis triggered by the high altitude.[54] The benefits of acute intermittent hypobaric hypoxia were also proved by Meeuwsen et al., where significant improvements were recorded in all important parameters of aerobic and anaerobic exercise tests (which the athletes were subjected to) at high altitudes, as compared to the sea level.[55]
In a research evaluating skeletal muscle changes after endurance training at high altitudes, the percentage of Type IIa fibers in the extensor digitorum longus muscle and deep portions of the plantaris muscle, as well as Type IIab fibers in fast-twitch muscles, was found to be enhanced. The muscles also showed marked metabolic adaptations, with increased activity levels of enzyme citrate synthase (involved in citric acid cycle) and 3 hydroxyacyl CoA dehydrogenase (beta-oxidation of fatty acids) and decreased lactate dehydrogenase activity, which overall proved to have a beneficial effect on them.[56]
Ten, it has been affirmed that Tibetan people have a better adaptation to high altitude since they have lived longer at high altitude and have a lower hematocrit than people from the Andes. Women have a lower hematocrit than man. Would this suggest that they are better adapted to life on planet earth? Man with a higher hematocrit and hemoglobin is well adapted also to the environment, and along with women forms the essential components of successful reproduction, thus far. It does seem evident, however, that women do live longer than men, being 122 years of age, as recorded and verified.[57]
It cannot be affirmed that we, the Andeans, are not well adapted to high altitude. It becomes evident that “Every living being according to the genetic buildup – that determines his species, race, and sex – has an optimal form of adaptation and the proof lies in the successful reproduction and survival at any altitude”– Prof Dr. Gustavo Zubieta-Calleja. Perhaps, this sentence presented during 2016 in high-altitude conferences can also include the term, longevity at high altitude. Several studies are needed to show if this trend is also evident in animals such as dogs, cats, and other species resident at high altitude. It is interesting to note that recent studies show that children who had pulmonary hypertension or high-altitude pulmonary hypertension (HAPH) in their youth and living at 3000 m in Colorado did not present pulmonary hypertension and comorbidities after 55 years, showing that there was long-term survival without comorbidities and that in some, there was a greater tendency to have exertional limitation, which in our criteria is not due to the HAPH, but to the underlying pulmonary disease that was not diagnosed and gave rise to the remodeling of HAPH.[58] But, this remodeling is merely an adaptive process following the adaptation formula where adaptation to high altitude = time/altitudeΔ[59] and reversible upon returning to sea level.
Eleven, high-altitude physicians and following the teachings of “sea-level high-altitude experts,” often advice people that get to a certain age in the city of La Paz and El Alto (3000–4100 m) to go down to live at a lower altitude. This erroneous assumption of “high-altitude deterioration of health” gives rise to social, economic, and familial conflicts due to this change at old age. Furthermore, many when they actually travel to lower altitude present other health problems, such as increased cholesterol, asthma, pneumonias, and several other complications that may in fact shorten their life span, without even mentioning the exposure to mosquito-transferred diseases described above. At our institute, with 46 years of experience, we never send anyone to lower altitudes, based solely on age. In fact, we hardly ever advice moving to lower altitudes.
The important element for life, oxygen, the subject of our analysis in relation to the decrease of the oxygen pressure at high altitude giving rise to hypobaric hypoxia was originally wrongly termed “oxygen” by Lavoisier as he mistakenly believed that it was a constituent of all acids, where “oxy” is the Greek root for “acids.” However, the name remained coined and became permanently established. Nevertheless, science has the obligation to clearly define or term certain biological alterations, as mistakes of interpretation can imperil the life of high-altitude residents. It is unacceptable that many genetic studies mistakenly include jointly many cardio-pulmonary, renal, carotid body, alterations of respiratory responses, hematological abnormalities, and many others in the search for genes that would explain the so-termed “de-adaptation,” or “loss of adaptation,” with which we are in full disagreement. We find stubbornness in trying to prove what is anti-natural. As expected, the labyrinth of findings of many genetic alterations is only creating more and more confusion and what is worse will delay the true understanding of the genetic favorable responses and perhaps “unfavorable” responses to hypoxia. If we consider that the physiology studied at sea level is the normal and acceptable way of living, we will never be able to understand life at high altitude, as a normal adaptation, and therefore we will never understand the development of life in the whole planet.
Chronic hypoxia provides humans with advantages over their sea-level counterparts, making them stronger and thereby extending their life span, as the organism becomes more resistant to hypoxia, a fundamental threat to survival. In fact, we strongly believe that sea-level residents carry the disability of poor tolerance to hypoxia that can shorten their lifespan.
Humans are preparing to become an interplanetary species, and the next move is the Mars space venture. Hypoxia will certainly be a menace and all the concepts herein expressed can be of great benefit to these futuristic evolutions. Human will have to cope with chronic hypoxia more and more.
All these observations help add up to the concept that chronic hypoxia is by no means deleterious to health and quite the contrary, in our criteria, favorable. We believe this so strongly that we have been proposing that space vehicles should have an environmental pressure similar to that of the city of La Paz (1/3rd lower than at sea level) that would give rise to many benefits including a lighter more manageable space suit.[60]
Conclusions
Longevity in Bolivians beyond 90 and 100 years of age is definitely extended in the high-altitude cities and departments. This implies that life and adaptation to life at high altitude is very successful in the hypobaric hypoxic environments. One of the best proofs that hypoxia is not necessarily deleterious is longevity at high altitude. Several variables could have influencing factors, but it seems evident that hypoxia per se, adaptation, and less ROS aggression as that suffered at sea level seem to play a fundamental favorable role. Sea-level residents have the disability of intolerance to hypoxia that grants high-altitude residents an advantage in the ultimate goal of life, longevity.
Acknowledgements
The authors express their most profound gratitude to the late Prof. Dr. Gustavo Zubieta-Castillo, our guiding mentor and innovative scientist that always questioned pre-established concepts, based on reason, logic and intuition, which with time have shown that he was right. Likewise, we want to express our gratitude to the late Prof. Poul-Erik Paulev, our friend and collaborator who unfortunately, passed away this year. We are also most thankful for the collaboration by Lucrecia De Urioste and Rafaela Zubieta De Urioste, for their constant support and suggestions and likewise assistance in bibliographic search and suggestions by AntaraBagchi, a most enthusiastic medical student from India, collaborating with us at IPPA. To Ing. Armando De Urioste for his advice on the statistical analyses and suggestions. Finally, to the SEGIP and its director, Ing Antonio Costas, for kindly providing a report with the information of the population >70 years of age, in Bolivia. We would like to thank our most distinguished scientist and friend Prof. Poul-Erik Paulev, for reading this article with his lovely wife Kirsten and sending us his approval. We also thank him for his guidance and teachings. Unfortunately, he passed away this year but he remains in our hearts forever.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.